2023 AEA Community Seed Grant Final Report: Dr. Alessandro Dinoto
May 29, 2026

It was August 15,2023 when we introduced Dr. Alessandro Dinoto. Click here for the introductory post where we learned about Dr. Dinoto, the study plans and how the project would help patients and families affected by AE.
In the 2023 AEA Community Seed Grant Final Report, Dr. Dinoto explains the outcomes of the project, Investigating the role of complement activation and antibody subclasses in anti-LGI1 and anti-CASPR2 encephalitis: a pilot study. (Final Report submitted October 2024)
1. List the specific aims of your project and explain how they were met.
The aims of this project were to develop live cell-based assays for LGI1 and CASPR2 antibodies, to categorize subclasses and study the role of complement in this disease potentially correlating it with clinical outcomes, when available. The rationale of this study is supported by evidence that complement-activating IgG1 subclasses are not found in all patients, but are associated, in some studies, with worst outcomes.
During this year we were able to develop and optimize live cell-based assays for the detection of LGI1 and CASPR2 antibodies. Antibody testing with live cell-based assays, compared to commercially available tests, allows a more precise diagnosis and allows to test in vitro the effect of autoantibodies on cells expressing the protein of interest.
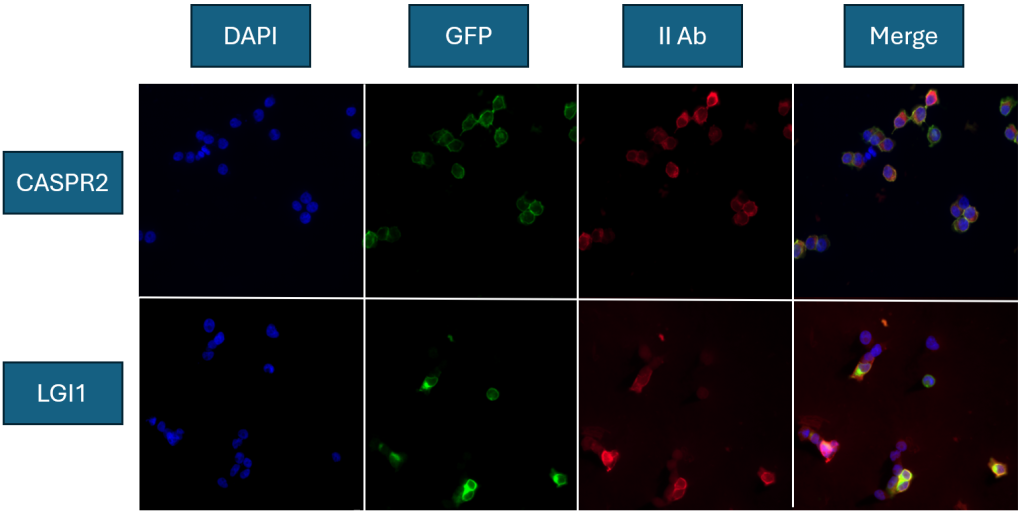
In particular, we developed an assay employing HEK293 cells transiently transfected with plasmid encoding GFP-tagged (a green marker) DNA codes for LGI1, ADAM23 and CASPR2 proteins for antibody detection. After transfection with these plasmids, cell transiently express LGI1 or CASPR2 on their surface. Serum samples are then incubated with these cells and, if there is an autoantibody against LGI1 or CASPR2, it binds the target. Then, a fluorescent (red marker) specific antibody is used for visualizing the presence of human antibodies. To help visualize cells, we also counterstain with DAPI, which shows the nuclei of cells (blue marker). Some examples of the assay for LGI1 and CASPR2 antibodies are reported in the attached figure. We validated these assays on multiple runs including positive and negative controls, to verify they worked properly before moving forward.
We have screened stored samples for LGI1 or CASPR2 positivity on commercial fixed cell-based assay from a single center and we retrieved n=14 CASPR2 and n=22 LGI1 patients with positive results, and then excluded n=3 CASPR2 and n=2 LGI1 being likely falsely positive after reviewing clinical data.
At this point, we have included 31 samples at disease onset from patients with a median age at onset of 65 years (range 35-82) and being 18 (60%) males. All patients have a clinical phenotype compatible with LGI1/CASPR2 antibodies, and full clinical data with outcomes are available for n=18 of them, so far.
After validating the cell-based assay, we have obtained the end point dilution of all LGI1 and CASPR2 positive samples (representing how much antibody is found in sera of patients) and we tested all samples for IgG4 subclasses, which resulted positive in all cases (as expected from previous studies), and obtained end point titers also for IgG4 subclass.
The current project is still ongoing, and we are working hard optimizing our IgG1 subclass assay, and we are developing the complement-dependent cytotoxicity assay, which would help determine if these antibodies are able to activate complement. Furthermore, we aim to expand our cohort including more patients once all assays have been validated.
2. Describe the proposed impact/relevance of the project and the outcome.
This project is still ongoing, and so far, we were able to establish and to validate a live cell-based assay for LGI1 and CASPR2 antibodies and obtained data for IgG4 subclasses. We are now working hard on optimizing the tests for IgG1 subclasses and for complement activation and we hope to enroll more patients, as we have reached the minimum sample size we had planned, but we believe that enrolling more patients would give more strength to this study.
3. Explain how the results of your project have direct implications for patients with AE.
We believe that studying complement may be relevant for patients with autoimmune encephalitis because it helps to understand how these antibodies cause damage to brain cells. The development of an assay for the detection of complement activity at disease onset could potentially be helpful to determine which patients will have a more severe disease, and also help clinicians identify those cases that require more intensive immunotherapy. Unfortunately, our data are still preliminary, and we cannot properly address these points, but we hope to have upcoming results soon.
4. How did the AEA Community Seed Grant contribute to your ability to complete this project
We are very thankful to the AEA Community for supporting our pilot study. Without the support from the Community, we would not be able to cover all costs related to the laboratory materials we are employing in the study and we could not start our journey.
Thank You, Thank You, Thank You!
Thank you, Dr. Dinoto, for your research and your commitment to improving the lives of patients and families impacted by AE.
Thank you to the entire AE Alliance Community for contributing during the 2023 Research Network Month which assisted in funding this seed grant project.
Thank you for your contributions this year to fund future research!
Together, we are changing the course of AE.
